Overview

We often think of fallen arches as a cause of foot pain, but they also stress your spine. In fact, fallen arches often contribute to unresolved or recurrent back pain. Excessive foot pronation (rolling in) can produce a short leg, pelvic unleveling, and increased curvature in your spine. Fallen arches place stress and strain on your feet, knees, hips, and spine. A custom orthotic can be a key part of your treatment plan in helping you get rid of your pain.
Causes
There are several reasons why arches fall. It can be genetic, it can be a result of unsupported shoes, a product of our lives and the pressure we put on the feet. Some people have active lifestyles so the wear and tear effect on the muscles there that runs down the back of the calf and wraps around the arch can slacken as we get older. It can be a number of things.
Symptoms
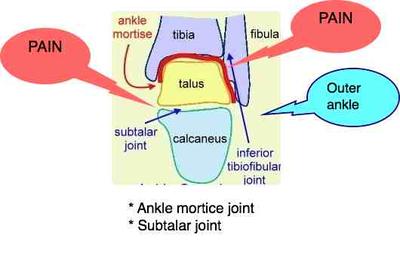
Pain along the inside of the foot and ankle, where the tendon lies. This may or may not be associated with swelling in the area. Pain that is worse with activity. High-intensity or high-impact activities, such as running, can be very difficult. Some patients can have trouble walking or standing for a long time. Pain on the outside of the ankle. When the foot collapses, the heel bone may shift to a new position outwards. This can put pressure on the outside ankle bone. The same type of pain is found in arthritis in the back of the foot. The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
Most children and adults with flatfeet do not need to see a physician for diagnosis or treatment. However, it is a good idea to see a doctor if the feet tire easily or are painful after standing, it is difficult to move the foot around or stand on the toes, the foot aches, especially in the heel or arch, and there is swelling on the inner side of the foot, the pain interferes with activity or the person has been diagnosed with rheumatoid arthritis. Most flatfeet are diagnosed during physical examination. During the exam, the foot may be wetted and the patient asked to stand on a piece of paper. An outline of the entire foot will indicate a flattened arch. Also, when looking at the feet from behind, the ankle and heel may appear to lean inward (pronation). The patient may be asked to walk so the doctor can see how much the arch flattens during walking. The doctor may also examine the patient's shoes for signs of uneven wear, ask questions about a family history of flatfeet, and inquire about known neurological or muscular diseases. Imaging tests may be used to help in the diagnosis. If there is pain or the arch does not appear when the foot is flexed, x-rays are taken to determine the cause. If tarsal coalition is suspected, computed tomography (CT scan) may be performed, and if an injury to the tendons is suspected, magnetic resonance imaging (MRI scan) may be performed.
flat feet exercises
Non Surgical Treatment
If you have flat feet, you may also experience pain throughout the lower body and into the lower back. Orthotics (custom-made rigid foot supports) can be prescribed when over-the-counter supports do not provide releif and surgery can also offer a more permanent solution in severe cases. The board-certified doctors in our practice would be able to select the most appropriate course of action in each case.
Surgical Treatment

Surgical correction is dependent on the severity of symptoms and the stage of deformity. The goals of surgery are to create a more functional and stable foot. There are multiple procedures available to the surgeon and it may take several to correct a flatfoot deformity. Stage one deformities usually respond to conservative or non-surgical therapy such as anti-inflammatory medication, casting, functional orthotics or a foot ankle orthosis called a Richie Brace. If these modalities are unsuccessful surgery is warranted. Usually surgical treatment begins with removal of inflammatory tissue and repair of the posterior tibial tendon. A tendon transfer is performed if the posterior tibial muscle is weak or the tendon is badly damaged. The most commonly used tendon is the flexor digitorum longus tendon. This tendon flexes or moves the lesser toes downward. The flexor digitorum longus tendon is utilized due to its close proximity to the posterior tibial tendon and because there are minimal side effects with its loss. The remainder of the tendon is sutured to the flexor hallucis longus tendon that flexes the big toe so that little function is loss. Stage two deformities are less responsive to conservative therapies that can be effective in mild deformities. Bone procedures are necessary at this stage in order to recreate the arch and stabilize the foot. These procedures include isolated fusion procedures, bone grafts, and/or the repositioning of bones through cuts called osteotomies. The realigned bones are generally held in place with screws, pins, plates, or staples while the bone heals. A tendon transfer may or may not be utilized depending on the condition of the posterior tibial tendon. Stage three deformities are better treated with surgical correction, in healthy patients. Patients that are unable to tolerate surgery or the prolonged healing period are better served with either arch supports known as orthotics or bracing such as the Richie Brace. Surgical correction at this stage usually requires fusion procedures such as a triple or double arthrodesis. This involves fusing the two or three major bones in the back of the foot together with screws or pins. The most common joints fused together are the subtalar joint, talonavicular joint, and the calcaneocuboid joint. By fusing the bones together the surgeon is able to correct structural deformity and alleviate arthritic pain. Tendon transfer procedures are usually not beneficial at this stage. Stage four deformities are treated similarly but with the addition of fusing the ankle joint.
We often think of fallen arches as a cause of foot pain, but they also stress your spine. In fact, fallen arches often contribute to unresolved or recurrent back pain. Excessive foot pronation (rolling in) can produce a short leg, pelvic unleveling, and increased curvature in your spine. Fallen arches place stress and strain on your feet, knees, hips, and spine. A custom orthotic can be a key part of your treatment plan in helping you get rid of your pain.
Causes
There are several reasons why arches fall. It can be genetic, it can be a result of unsupported shoes, a product of our lives and the pressure we put on the feet. Some people have active lifestyles so the wear and tear effect on the muscles there that runs down the back of the calf and wraps around the arch can slacken as we get older. It can be a number of things.
Symptoms
Pain along the inside of the foot and ankle, where the tendon lies. This may or may not be associated with swelling in the area. Pain that is worse with activity. High-intensity or high-impact activities, such as running, can be very difficult. Some patients can have trouble walking or standing for a long time. Pain on the outside of the ankle. When the foot collapses, the heel bone may shift to a new position outwards. This can put pressure on the outside ankle bone. The same type of pain is found in arthritis in the back of the foot. The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
Most children and adults with flatfeet do not need to see a physician for diagnosis or treatment. However, it is a good idea to see a doctor if the feet tire easily or are painful after standing, it is difficult to move the foot around or stand on the toes, the foot aches, especially in the heel or arch, and there is swelling on the inner side of the foot, the pain interferes with activity or the person has been diagnosed with rheumatoid arthritis. Most flatfeet are diagnosed during physical examination. During the exam, the foot may be wetted and the patient asked to stand on a piece of paper. An outline of the entire foot will indicate a flattened arch. Also, when looking at the feet from behind, the ankle and heel may appear to lean inward (pronation). The patient may be asked to walk so the doctor can see how much the arch flattens during walking. The doctor may also examine the patient's shoes for signs of uneven wear, ask questions about a family history of flatfeet, and inquire about known neurological or muscular diseases. Imaging tests may be used to help in the diagnosis. If there is pain or the arch does not appear when the foot is flexed, x-rays are taken to determine the cause. If tarsal coalition is suspected, computed tomography (CT scan) may be performed, and if an injury to the tendons is suspected, magnetic resonance imaging (MRI scan) may be performed.
flat feet exercises
Non Surgical Treatment
If you have flat feet, you may also experience pain throughout the lower body and into the lower back. Orthotics (custom-made rigid foot supports) can be prescribed when over-the-counter supports do not provide releif and surgery can also offer a more permanent solution in severe cases. The board-certified doctors in our practice would be able to select the most appropriate course of action in each case.
Surgical Treatment
Surgical correction is dependent on the severity of symptoms and the stage of deformity. The goals of surgery are to create a more functional and stable foot. There are multiple procedures available to the surgeon and it may take several to correct a flatfoot deformity. Stage one deformities usually respond to conservative or non-surgical therapy such as anti-inflammatory medication, casting, functional orthotics or a foot ankle orthosis called a Richie Brace. If these modalities are unsuccessful surgery is warranted. Usually surgical treatment begins with removal of inflammatory tissue and repair of the posterior tibial tendon. A tendon transfer is performed if the posterior tibial muscle is weak or the tendon is badly damaged. The most commonly used tendon is the flexor digitorum longus tendon. This tendon flexes or moves the lesser toes downward. The flexor digitorum longus tendon is utilized due to its close proximity to the posterior tibial tendon and because there are minimal side effects with its loss. The remainder of the tendon is sutured to the flexor hallucis longus tendon that flexes the big toe so that little function is loss. Stage two deformities are less responsive to conservative therapies that can be effective in mild deformities. Bone procedures are necessary at this stage in order to recreate the arch and stabilize the foot. These procedures include isolated fusion procedures, bone grafts, and/or the repositioning of bones through cuts called osteotomies. The realigned bones are generally held in place with screws, pins, plates, or staples while the bone heals. A tendon transfer may or may not be utilized depending on the condition of the posterior tibial tendon. Stage three deformities are better treated with surgical correction, in healthy patients. Patients that are unable to tolerate surgery or the prolonged healing period are better served with either arch supports known as orthotics or bracing such as the Richie Brace. Surgical correction at this stage usually requires fusion procedures such as a triple or double arthrodesis. This involves fusing the two or three major bones in the back of the foot together with screws or pins. The most common joints fused together are the subtalar joint, talonavicular joint, and the calcaneocuboid joint. By fusing the bones together the surgeon is able to correct structural deformity and alleviate arthritic pain. Tendon transfer procedures are usually not beneficial at this stage. Stage four deformities are treated similarly but with the addition of fusing the ankle joint.




 Morton?s neuroma is a swollen nerve in the distal portion of the foot. The enlarged portion of the nerve represents scarring within the plantar nerve that occurs after chronic compression and/or repetitive injury. This may come about when the toes are squeezed together for too long, as can occur with the chronic use of high heels. The nerve that runs between your toes will swell and thicken. This can cause pain when walking. The symptoms of Morton?s neuroma can include burning pain in the foot, the feeling of a lump inside your foot, pain between the third and fourth toes typically but it can occur between other toes.
Morton?s neuroma is a swollen nerve in the distal portion of the foot. The enlarged portion of the nerve represents scarring within the plantar nerve that occurs after chronic compression and/or repetitive injury. This may come about when the toes are squeezed together for too long, as can occur with the chronic use of high heels. The nerve that runs between your toes will swell and thicken. This can cause pain when walking. The symptoms of Morton?s neuroma can include burning pain in the foot, the feeling of a lump inside your foot, pain between the third and fourth toes typically but it can occur between other toes.



 Achilles tendinosis (also known as Achilles tendinopathy) is a soreness and stiffness that comes on gradually and continues to worsen until treated. It is a common injury among middle and long distance runners. The severity of Achilles tendinosis can be broken down into four stages, each of which can be measured in terms of how the Achilles tendon feels during exercise, the amount of stiffness and creaking, and Achilles tendon?s soreness to the touch (the Achilles tendon pinch test). The four stages, or grades, are, No pain during exercise, but there is some discomfort in the morning when first getting out of bed. The stiffness and creaking go away after a few minutes and are fine the rest of the day. Lightly pinching the Achilles tendon with the forefinger and thumb in the morning or after exercise will probably indicate soreness. Pain during exercise or running, but performance is not affected. The stiffness and creaking continue to appear when first getting out of bed and continue to disappear shortly afterward. Lightly pinching the Achilles tendon with the forefinger and thumb in the morning or after exercise will indicate soreness. Pain during exercise or running that is detrimental to performance. The stiffness and creaking continue to appear when first getting out of bed, but may continue for some time and reappear at other points during the day. Lightly pinching the Achilles tendon with the forefinger and thumb in the morning or after exercise will indicate soreness. Hurts too much to exercise or run. The stiffness and creaking continue to appear when first getting out of bed, but may continue for most of the day. Lightly pinching the Achilles tendon with the forefinger and thumb at almost any time of day will indicate soreness.
Achilles tendinosis (also known as Achilles tendinopathy) is a soreness and stiffness that comes on gradually and continues to worsen until treated. It is a common injury among middle and long distance runners. The severity of Achilles tendinosis can be broken down into four stages, each of which can be measured in terms of how the Achilles tendon feels during exercise, the amount of stiffness and creaking, and Achilles tendon?s soreness to the touch (the Achilles tendon pinch test). The four stages, or grades, are, No pain during exercise, but there is some discomfort in the morning when first getting out of bed. The stiffness and creaking go away after a few minutes and are fine the rest of the day. Lightly pinching the Achilles tendon with the forefinger and thumb in the morning or after exercise will probably indicate soreness. Pain during exercise or running, but performance is not affected. The stiffness and creaking continue to appear when first getting out of bed and continue to disappear shortly afterward. Lightly pinching the Achilles tendon with the forefinger and thumb in the morning or after exercise will indicate soreness. Pain during exercise or running that is detrimental to performance. The stiffness and creaking continue to appear when first getting out of bed, but may continue for some time and reappear at other points during the day. Lightly pinching the Achilles tendon with the forefinger and thumb in the morning or after exercise will indicate soreness. Hurts too much to exercise or run. The stiffness and creaking continue to appear when first getting out of bed, but may continue for most of the day. Lightly pinching the Achilles tendon with the forefinger and thumb at almost any time of day will indicate soreness.




 RSS Feed
RSS Feed
